Research Insights
Does Medicaid Reimbursement Impact Immediate Postpartum Long-Acting Reversible Contraceptive Use?
Key Takeaway
Medicaid reimbursement of immediate postpartum long-acting reversible contraception (LARC) increased the use of LARC provided in hospitals following childbirth in Georgia, Iowa, Maryland, New York, and Rhode Island. The increases in use were concentrated in a small subset of hospitals that were less likely to be rural or Catholic-owned. This study’s results may be of particular interest to state Medicaid agencies considering adopting similar payment policies and to inform efforts to improve LARC availability and use across hospitals and providers in states that already offer reimbursement.
Why This Study Is Important
Researchers found that a policy change to Medicaid reimbursement for immediate postpartum LARC, including implantable contraception or intrauterine devices (IUDs), was associated with an increase in LARC use during postpartum hospital stays. This is significant given that over half of US states have implemented this policy. Previously, the lack of reimbursement limited inpatient access and availability. As Medicaid pays for roughly 42% of childbirth hospitalizations annually, such payment policies have important implications. Continuing to improve coverage for LARC may reduce the adverse maternal and child health outcomes associated with short-interval pregnancies that occur within the first six months post-childbirth and are largely unplanned. Understanding policy effectiveness is key as other states assess their own policies or consider adopting similar practices.
What This Study Found
Researchers studied 1,521,491 Medicaid-paid births and 1,575,697 commercially-paid births across Georgia, Iowa, Maryland, New York, and Rhode Island between 2011 and 2017.
- Medicaid reimbursement for immediate postpartum LARC was associated with increases in use among Medicaid-paid births.
- Across all study states, the rate of immediate postpartum LARC placement increased significantly after the policy change.
- By the end of the study period (2017), the policy had increased overall immediate postpartum LARC use in four of the states studied. Effects varied across states, with an increase of 1.88 percentage points (ppts) in Georgia, 0.38 ppts in Maryland, 2.27 ppts in New York, and 9.15 ppts in Rhode Island.
- Across all study states, the increase in immediate postpartum LARC use after the policy change was concentrated in a small subset of hospitals. Most hospitals (73%) provided no immediate postpartum LARC following Medicaid-paid childbirths.
- Hospitals that provided immediate postpartum LARC were more likely to be urban and to be teaching hospitals providing the highest level of obstetric care. They were also less likely to be owned or affiliated with a Catholic organization.
- Researchers also found that the use of immediate postpartum LARCs after commercially-paid births increased modestly in four of the five states after the policy change (all except Iowa).
What These Findings Mean
Medicaid reimbursement for immediate postpartum LARC is an effective tool for providing contraception access but further efforts are needed to increase adoption across hospitals and providers. Policy implementation has been uneven which may contribute to within-state inequities, especially in rural areas or those served by Catholic-owned hospitals. It remains important to understand within-state differences to promote wider uptake across hospitals. In addition, this policy increases the convenience and effectiveness of contraceptive options prior to hospital discharge, but it is imperative that care is also patient-centered to ensure contraceptive autonomy.
More About This Study
This longitudinal study examined the impact of Medicaid reimbursement policy changes on immediate postpartum LARC uptake. Using data available through the Healthcare Cost and Utilization Project (HCUP), researchers were able to investigate the policy’s effect in states whose Medicaid programs implemented reimbursement changes between 2014 and 2015 and had inpatient data available from 2011 to 2017. In four states (all except Georgia), HCUP hospital discharge data were linked to the American Hospital Association’s Annual Survey which enabled identification of facility teaching and rural status, Catholic affiliation, and obstetric level of care. LARC billing codes were adapted from the Office of Population Affairs to create an indicator for receipt of an immediate postpartum LARC. An interrupted time series design was used to estimate the extent to which the Medicaid reimbursement change impacted provision of immediate postpartum LARC. Each state was analyzed separately at the hospital-quarter level.
Steenland MW, Vatsa R, Pace LE, & Cohen JL. Immediate Postpartum Long-Acting Reversible Contraceptive Use Following State-Specific Changes in Hospital Medicaid Reimbursement. JAMA Network Open. 2022;5(10):e2237918. doi:10.1001/jamanetworkopen.2022.37918
For more information about this study, contact Jessica Cohen at cohenj@hsph.harvard.edu. For more information about the NIHCM Foundation Investigator-Initiated Research Grant Program, contact Cait Ellis at cellis@nihcm.org.
Research Insights
Published on: March 31, 2022.
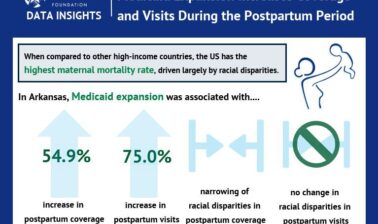
Does Medicaid Expansion Impact Postpartum Coverage, Outpatient Visits, and Racial Disparities?
More About This Grantee

Get nihcm updates
Updates on timely topics and webinars delivered to your inbox
More Related Content
See More on: Health Care Coverage | Health Care Reform | Maternal and Child Health